Home / Articles
Cervical vs. Lumbar Herniated Disc: Which One Do You Have?
Home / Articles
Cervical vs. Lumbar Herniated Disc: Which One Do You Have?
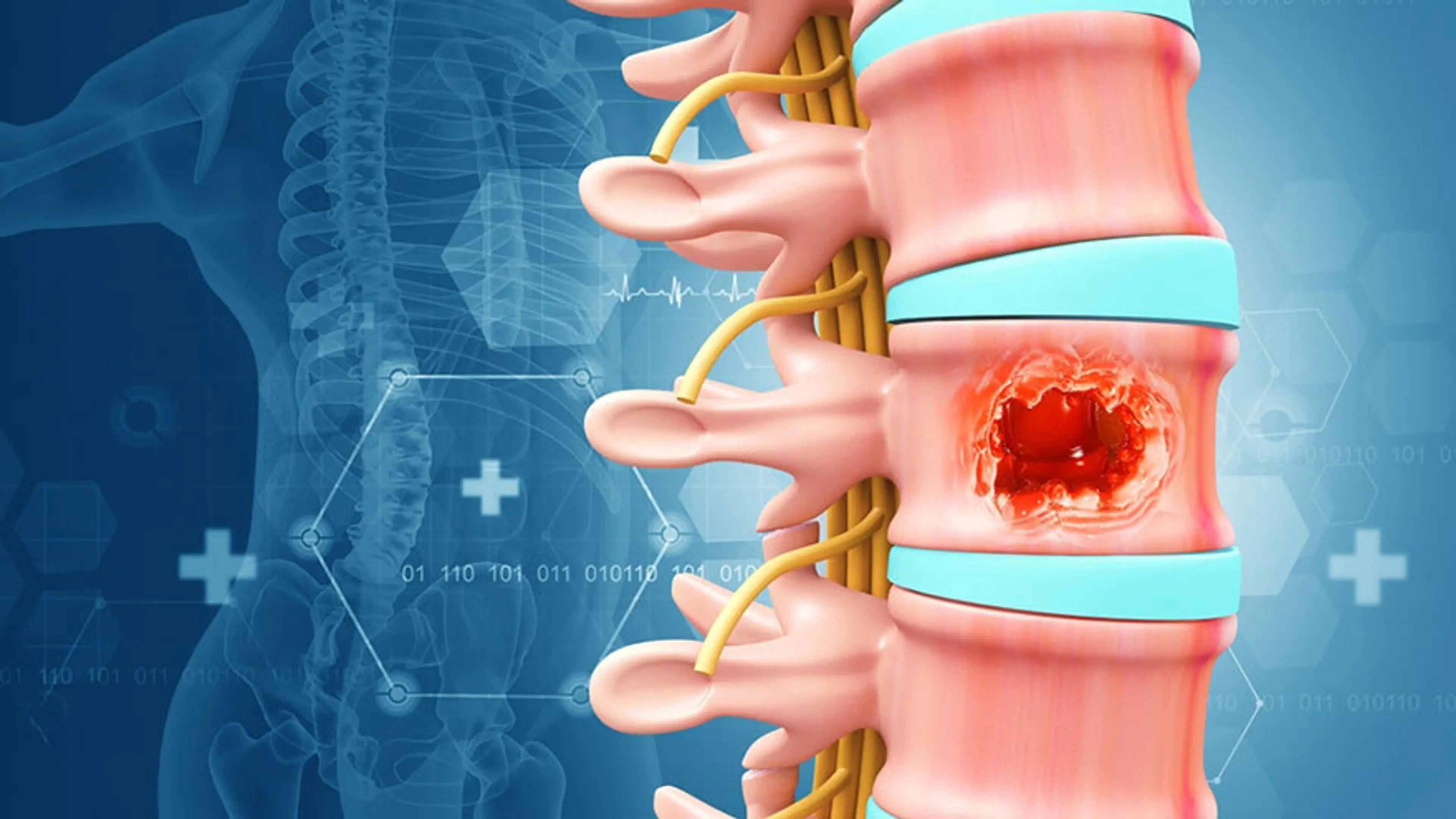
Between each spinal bone sits an intervertebral disc. These discs are designed to absorb shock, distribute load, and allow smooth spinal movement. Each disc consists of:
A tough outer layer that provides structural integrity
A softer, gel-like inner core that absorbs pressure
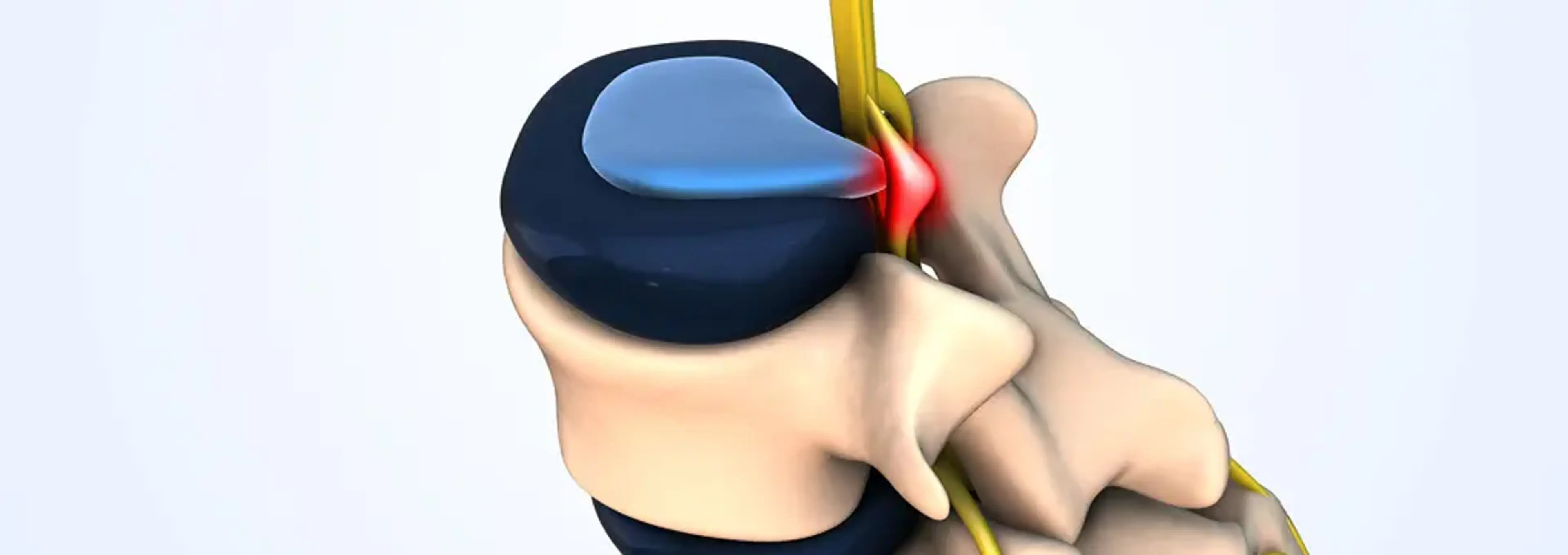
The exact symptoms depend on:
Which spinal level is affected
Which nerve root is compressed
How sensitive the nerve has become over time
This is why two people with “disc herniation” can have completely different experiences—and why identifying the location is more important than focusing on the MRI wording alone.
The cervical spine consists of seven vertebrae (C1–C7) supporting the head and connecting the brain to the rest of the body. Nerves exiting this region travel into the shoulders, arms, and hands, and also contribute to balance, coordination, and fine motor control.
Because the cervical spine must remain mobile while supporting the weight of the head, it is particularly sensitive to posture-related stress. Even a small disc herniation in this area can produce noticeable neurological symptoms.
Patients with cervical disc herniation often report:
Neck pain or stiffness, especially with movement
Pain spreading into one shoulder or down one arm
Tingling, numbness, or burning sensations in the fingers
Weak grip strength or clumsiness in the hand
A heavy, fatigued feeling in the arms
Headaches that begin at the base of the skull and radiate forward
In everyday clinical practice, cervical disc herniation is closely linked to modern lifestyle patterns, especially in urban Korean populations. Common contributors include:
Prolonged smartphone use with the head tilted forward
Desk work with monitors positioned too low
Long commutes spent sitting and looking down
Chronic stress leading to persistent neck and shoulder muscle tension
Over time, forward head posture increases the mechanical load on the lower cervical discs. This added stress accelerates disc degeneration and increases the likelihood of nerve compression. Many patients are unaware of these changes until symptoms begin to interfere with daily tasks like typing, driving, or sleeping.
The lumbar spine (L1–L5) supports most of the body’s weight and manages powerful movements such as bending, lifting, and prolonged sitting. Nerves from this region travel through the buttocks, thighs, legs, and feet, supplying both sensation and muscle control.
Because of the heavy mechanical demands placed on it, the lumbar spine is the most common site of disc herniation.
Lumbar disc herniation typically presents with:
Lower back pain that may come and go
Pain radiating down one leg, often referred to as sciatica
Numbness or tingling in the thigh, calf, or foot
Muscle weakness that affects walking or stair climbing
Difficulty standing up after sitting for a long time
Pain that worsens with sitting, bending forward, or prolonged driving
This happens because nerve compression in the lumbar spine frequently irritates the sciatic nerve, which carries pain signals far from the original source.
Most patients with lumbar disc herniation share long-term stress patterns rather than a single injury. These often include:
Prolonged sitting without adequate lumbar support
Weak core and hip stabilizing muscles
Repeated bending or lifting with poor mechanics
Old back injuries that were never fully rehabilitated
Limited daily movement and physical conditioning
In many cases, lumbar disc herniation represents the final stage of years of accumulated strain rather than a sudden accident.
Category | Cervical Disc (Neck) | Lumbar Disc (Lower Back) |
|---|---|---|
Main pain location | Neck, shoulder, arm | Lower back, buttock, leg |
Nerve symptoms | Arm/hand tingling or weakness | Leg/foot tingling or weakness |
Typical pain spread | Down the arm | Down the leg |
Common triggers | Phone use, desk posture | Sitting, bending, lifting |
Balance effects | Sometimes affected | Rare |
Daily limitations | Work, driving, sleep | Walking, sitting, standing |
This distinction is often the first step in narrowing down the correct diagnosis and avoiding unnecessary or ineffective treatments.
One of the most important conversations we have with patients is this:
In real clinical practice, it is common to find:
Large herniations in patients with minimal symptoms
Small disc bulges causing severe nerve pain
Multiple abnormal discs, with only one being clinically relevant
MRI is a powerful diagnostic tool, but it must be interpreted alongside:
A detailed neurological examination
Careful symptom correlation
Posture and gait analysis
Functional movement assessment
Many patients arrive anxious after reading their MRI report, assuming surgery is inevitable. Most feel relieved once they understand that imaging findings alone do not determine treatment decisions.
At Yonsei Baro Walk Clinic, care typically focuses on:
Individualized rehabilitation programs tailored to symptoms
Posture and gait correction to reduce spinal stress
Nerve-focused pain management strategies
Ultrasound-guided injections when clinically indicated
Regenerative options such as PRP in selected cases
Practical changes to daily habits, workstations, and movement patterns
The objective is not just to reduce pain, but to address the underlying causes that led to disc overload. Pain relief without movement correction often results in recurrence.
You do not need to diagnose yourself, but these questions can help guide your understanding:
Does your pain travel into your arm or into your leg?
Do finger symptoms worsen when you move your neck?
Does sitting make leg pain worse than standing or walking?
Do you notice weakness or coordination changes, not just pain?
Have your posture or daily habits changed over the years?
If your symptoms feel unclear or overlap, that is common. Disc-related nerve pain does not always follow textbook patterns, which is why individualized assessment is essential.
One of the most common misunderstandings about disc problems is assuming the disc itself is the sole issue. In reality, pain usually develops from a combination of posture, repetitive movement habits, muscle imbalance, and increasing nerve sensitivity—building quietly over time.
At Yonsei Baro Walk Clinic, we believe meaningful recovery begins with clarity, precise diagnosis, and care that treats the whole person—not just the MRI image.